

Tirzepatide outperforms other GLP-1 drugs in diabetes for blood sugar and weight loss
Key Takeaways:
- Tirzepatide demonstrated the strongest reductions in HbA1c and body weight among all GLP-1 RAs analysed, outperforming even Semaglutide and Liraglutide.
- Gastrointestinal side effects were common across long-acting agents, while hypoglycaemia risk varied, with Liraglutide offering a safer profile for some individuals.
- The findings reinforce a clinical shift towards long-acting and dual agonist therapies for managing type 2 diabetes, offering guidance for clinicians, payers, and policymakers.
Growing burden of type 2 diabetes drives search for optimal treatments
Every ten seconds, someone around the globe develops type 2 diabetes mellitus (T2DM) — a chronic disease that substantially raises household healthcare costs and doubles the risk of cardiovascular events such as heart attacks. The worldwide prevalence is projected to soar to 643 million by 2030, intensifying the need for treatments that lower blood glucose levels without contributing to weight gain.
Glucagon-like peptide-1 receptor agonists (GLP-1 RAs) both stimulate insulin secretion and suppress appetite. However, with a crowded marketplace of differing doses, formulations, and costs, families, clinicians, and health systems continue to seek the medication that offers maximum benefit with minimal drawbacks. This underscores the importance of robust comparative studies.
Rigorous study design to compare eight GLP-1 RAs
In a comprehensive study recently published in Scientific Reports, researchers undertook a systematic review and Bayesian network meta-analysis (NMA) to evaluate the glycaemic, weight, cardiovascular, and safety outcomes of eight GLP-1 RAs. The analysis compared these agents to placebo and standard antidiabetic drugs in adults living with T2DM.
The review adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses for Network Meta-Analyses (PRISMA-NMA) guidelines and was registered with the International Prospective Register of Systematic Reviews. The research team systematically searched PubMed, Cochrane Library, Embase, Web of Science, and Chinese databases up to 2 October 2024.
Eligible studies were randomised controlled trials (RCTs) lasting at least eight weeks, involving adults with T2DM. These trials compared twice-daily Exenatide (EBID), once-weekly Exenatide (EQW), Semaglutide, Albiglutide, Lixisenatide, Dulaglutide, Liraglutide, or Tirzepatide against each other, placebo, or traditional antidiabetic agents such as insulin, metformin, sodium-dependent glucose transporter 2 (SGLT2) inhibitors, dipeptidyl peptidase-4 (DPP-4) inhibitors, or sulfonylureas.
For analysis, oral and injectable Semaglutide were grouped due to their comparable efficacy. Independent reviewers conducted study selection, data extraction, and Cochrane risk-of-bias assessments, resolving any differences through consensus.
Outcomes assessed and statistical approach
The primary outcomes were changes from baseline in glycosylated haemoglobin A1c (HbA1c) and fasting plasma glucose (FPG). Secondary outcomes included changes in body weight, body mass index (BMI), systolic and diastolic blood pressure (SBP, DBP), total cholesterol (TC), high-density and low-density lipoprotein cholesterol (HDL-C, LDL-C), and reported adverse events.
Mean differences (MD) or risk ratios (RR) were calculated with 95% confidence intervals (CIs). When heterogeneity exceeded 50% (as measured by I²), a random-effects model was applied, with Chi-squared tests used to quantify variability.
Tirzepatide shows leading benefits in blood glucose and weight outcomes
From 64 eligible trials involving 25,572 participants, a dense evidence network emerged. Compared with placebo, all GLP-1 RAs lowered HbA1c, but the extent varied markedly:
- Tirzepatide achieved the largest absolute HbA1c reduction (MD −2.3 percentage points; 95% CI −2.7 to −1.9), followed by Semaglutide (−1.5) and Liraglutide (−1.2).
- Lixisenatide’s modest reduction of −0.56 placed it last.
When compared to a pooled group of conventional drugs (including insulin, metformin, SGLT2 inhibitors, DPP-4 inhibitors, and sulfonylureas), only Tirzepatide (−1.5), Semaglutide (−0.73), Liraglutide (−0.40), Dulaglutide (−0.34), and EQW (−0.36) demonstrated statistically significant superiority.
A similar hierarchy was evident for FPG reductions: Tirzepatide lowered FPG by −3.1 mmol/L, followed by Semaglutide (−2.0) and Liraglutide (−1.6). Short-acting agents and Albiglutide offered negligible improvements. The Surface Under the Cumulative Ranking Curve analysis gave Tirzepatide a 100% probability of being the top agent for glycaemic outcomes.
Marked differences in weight outcomes
The weight loss data revealed even starker contrasts. Compared to placebo:
- Tirzepatide achieved a striking −9.1 kg reduction,
- Semaglutide −2.8 kg,
- EBID −1.8 kg, and
- Liraglutide −1.2 kg.
Notably, EBID outperformed Liraglutide in this comparison. When benchmarked against traditional drugs, all GLP-1 RAs except Albiglutide reduced weight, with Dulaglutide and Lixisenatide also showing meaningful effects. Tirzepatide again led with a −10 kg difference.
Changes in blood pressure, BMI, and lipid fractions did not reach statistical significance across interventions, suggesting that glucose and weight benefits did not yet translate into short-term shifts in these cardiovascular parameters.
Safety profile: balancing gastrointestinal effects and hypoglycaemia risk
Gastrointestinal side effects were the most common adverse events. Compared with placebo:
- Semaglutide, Dulaglutide, Liraglutide, Lixisenatide, and Tirzepatide each tripled the risk of nausea and vomiting.
- However, when compared to older drugs already known for gastrointestinal intolerance, the risks were similar.
Hypoglycaemia risk varied considerably:
- EBID and Semaglutide significantly increased episodes (RR 3.3 and 4.6, respectively) versus placebo.
- In contrast, Liraglutide and Lixisenatide actually reduced hypoglycaemia risk compared with traditional regimens, highlighting a possible advantage for people prone to low blood sugar.
Other side effects, such as nasopharyngitis, headache, and elevated lipase levels, showed no material differences. Robust statistical checks (node-splitting, loop inconsistency tests) found no significant discrepancies between direct and indirect comparisons, and funnel plots suggested low publication bias.
Clinical implications and concluding remarks
This analysis positions Tirzepatide as the most effective agent overall for lowering blood glucose and achieving weight loss, with Semaglutide as a reliable second choice. As the authors note, Tirzepatide’s dual agonist activity at GIP and GLP-1 receptors likely underpins its superior outcomes.
Meanwhile, Liraglutide offers moderate glucose improvements with the least risk of hypoglycaemia, potentially making it preferable for leaner adults or those at risk of underweight and frequent hypoglycaemic episodes.
Short-acting formulations and Albiglutide rarely dominated in any category, emphasising the current shift towards once-weekly or dual agonist therapies. Sensitivity and subgroup analyses confirmed these rankings, increasing their practical relevance.
For clinicians, these findings offer valuable guidance in tailoring treatment to individual needs — balancing glucose targets, weight goals, gastrointestinal tolerance, and hypoglycaemia risk. For policymakers and payers, prioritising agents like Tirzepatide or Semaglutide may provide the best outcomes for people with obesity-related diabetes, while reserving Liraglutide for specific patient profiles.
Read More
Global study suggests universal GLP-1 access could halve obesity rates and save millions of lives in five years
Key Takeaways:
- Universal access to GLP-1 receptor agonists could reduce global obesity prevalence by around 52%, potentially improving the health of more than half a billion people.
- A large-scale microsimulation study estimated that such access could prevent approximately 37.5 million deaths over a five-year period by lowering all-cause mortality by nearly 7%.
- Researchers hope these findings will encourage international policy efforts to improve availability and affordability of GLP-1 treatments.
Ambitious modelling seeks to quantify global impact
Universal access to GLP-1 receptor agonists (GLP-1RAs) for eligible people could dramatically cut global obesity rates by half and save tens of millions of lives over just five years, according to new research presented by Elizabeth Staton, a doctoral candidate at Emory University’s Rollins School of Public Health.
“There has been a lot of interest in GLP-1s and how they seem so effective and widely beneficial, but it wasn’t yet quantified what would be that impact on a global level,” Staton told Healio. “We found a probability study … [but] it wasn’t very rigorous.”
Seeking to close this gap, Staton and her team constructed a detailed microsimulation model to predict the worldwide effect of offering GLP-1 therapies such as semaglutide (marketed as Ozempic, Wegovy and Rybelsus by Novo Nordisk) to all eligible individuals. Their work was unveiled during a presentation at a major conference.
The GEM model – a vast global microsimulation
Staton developed what she termed the GEM model (Global Epidemiology Multimorbidity microsimulation model), building on the established Bravo diabetes model created by her colleague Hui Shao, PhD, at the Emory Global Diabetes Research Center.
“I work in a research group in the Emory Global Diabetes Research Center with Hui Shao, PhD, who has a very well-validated Bravo model of diabetes complications. Stemming from that, I’ve created a global epidemiology multimorbidity microsimulation model, which we call the GEM model. This uses peer-reviewed studies for risk ratios, … So then our estimates are slightly more rigorous,” Staton explained.
The study encompassed a synthetic population of roughly 6.57 billion individuals aged 12 years and older, using detailed health data from the 2021 Global Burden of Disease and Non-Communicable Disease Risk Factor Collaboration studies. Eligibility for treatment was defined as having obesity and being at least 12 years old, or having type 2 diabetes with overweight and being at least 18 years old.
“Because it’s a microsimulation, we have individual level data, so we can just subset into people who would fit in the cohort studies. Then we compare our estimates that are predicted vs. the actual cohort studies,” Staton said.
The researchers validated their model by comparing it with prospective cohort studies and existing probability models to ensure robust estimates.
Striking findings on obesity and mortality
The results were remarkable. Staton and colleagues estimated that more than 1 billion people worldwide meet the criteria for semaglutide treatment. Under a scenario of universal access:
- Global obesity prevalence would decline by approximately 52%, an absolute reduction of about 9 percentage points, potentially improving the lives of around 565 million people.
- All-cause mortality would fall by nearly 7%, an absolute reduction of 0.6 percentage points, preventing an estimated 37.5 million deaths within five years.
“The compelling finding is that obesity would be reduced by almost 50% [and] mortality reduced by about 7% globally. These are hugely impactful [estimations] in just a 5-year time horizon,” Staton emphasised.
Hopes for policy and pricing changes
Staton hopes that these findings will help spur global efforts to expand access to GLP-1 therapies. “I hope these data move the conversation about global access forward. There are a number of reasons why access to GLP-1s are limited, with costs, supply and access to providers who prescribe them,” she told Healio.
Ultimately, she hopes that evidence of such a substantial potential benefit might encourage policymakers, manufacturers and global health agencies to invest more heavily in reducing drug costs and expanding prescribing infrastructure.
A tool for thought – not an immediate roadmap
Despite the eye-catching figures, Staton cautioned that this microsimulation is not intended as a direct prediction of what will happen. “The joy of microsimulation is that it’s not really a realistic scenario, but it’s an interesting one to explore,” she said.
Even so, the research underscores the scale of potential benefits if barriers to GLP-1 access could be overcome – offering a powerful data-driven argument for rethinking the global approach to obesity and metabolic disease treatment.
CCH Insight:
The potential benefits of GLP-1 receptor agonists and other, similar, anti-obesity medications are indeed huge, and possibly much greater than predicted in this study, due to the wide-ranging impact of these medicines. Not only do they treat obesity, they also improve glycaemic control and reduce cardiovascular disease risk, and may also protect against liver disease, kidney disease and neurodegenerative diseases like Parkinson’s and dementia.
Read More
Novo Nordisk expands digital health partnerships to enhance GLP-1RA weight loss outcomes
Key Takeaways:
- Novo Nordisk launches the Novo Nordisk Partner Platform to integrate digital tools into the care pathway for individuals using semaglutide (Wegovy) for weight loss.
- The initiative seeks collaborations with AI-powered nutrition apps, body composition scanners, telehealth services, and pharmacies to improve clinical outcomes.
- The company aims to consolidate its leadership in the global weight loss market amidst growing competition from Eli Lilly and expanding its obesity pipeline beyond GLP-1 receptor agonists.
Strategic Expansion Through Digital Integration
Novo Nordisk has unveiled a new initiative designed to enhance the weight loss outcomes of people receiving treatment with its glucagon-like peptide-1 receptor agonist (GLP-1RA), semaglutide, marketed as Wegovy for obesity and Ozempic for type 2 diabetes. The company is now seeking partnerships with digital health innovators across all stages of the weight management journey to better support individuals in achieving and maintaining clinically significant weight loss.
This effort is being formalised through the Novo Nordisk Partner Platform (NNPP), announced at the HLTH Europe conference in Amsterdam, held from 16 to 19 June. The announcement was made by Anne Cathrine Fleischer, Vice President of Global Obesity Consumer Engagement and New Business Models at Novo Nordisk.
A Digital Ecosystem for Personalised Support
Fleischer described the NNPP as a strategy to build a “marketplace of selected solutions” designed to complement pharmacological treatment with digital support. “The idea is that we create this ecosystem or marketplace of selected solutions that people can pick and choose from, so when a patient has started treatment, we know they have received help,” she said.
She continued: “We know when we look at our own digital tools that when intervention is combined with those efficient weight loss medications, patients are receiving better weight loss, so we hope we can significantly improve outcomes by combining education with digital tools.”
Through this platform, individuals prescribed semaglutide for weight management will gain access to additional services such as exercise coaching and nutritional guidance, either via the Novo Nordisk website or its Novo Care platform. The company is also exploring the development of a consolidated mobile application to house these resources in one accessible interface.
Targeting Muscle Loss and Optimising Nutrition
A particular focus for the company is addressing muscle mass loss, a known issue associated with GLP-1RA therapies. Novo Nordisk is in discussions with a technology partner whose AI-powered application can scan a person’s plate of food and assess whether it meets their nutritional requirements – especially protein intake.
In addition, the company is exploring collaborations with developers of mobile apps that scan body composition, allowing individuals to monitor changes in lean mass and fat distribution throughout their treatment.
Broader Partnerships to Enhance the Care Pathway
In a bid to offer more integrated care, Novo Nordisk is also seeking partnerships with telehealth providers and community pharmacies to deliver accessible medical advice to people receiving GLP-1RA treatment. “By partnering with these players, we can provide a much better patient journey and care pathway,” Fleischer added.
The company’s approach reflects a broader ambition to deliver not just medication, but a holistic model of obesity care that supports long-term behavioural change and health outcomes.
Advancing the Competitive Edge in Obesity Care
Novo Nordisk’s push into digital health partnerships comes as it faces growing competition from Eli Lilly. Earlier this year, Lilly’s dual agonist Zepbound (tirzepatide) demonstrated superior weight loss outcomes to Wegovy in a Phase III clinical trial. Novo Nordisk is responding by accelerating the development of its next-generation therapies.
In early June, the company announced that it had moved both subcutaneous and oral formulations of amycretin into Phase III trials for people living with obesity or overweight. It has also launched two additional Phase III trials of CagriSema, another pipeline candidate.
Further, Novo Nordisk has strengthened its drug discovery capabilities through an $812 million partnership with Deep Apple Therapeutics, aimed at identifying novel small molecules for obesity and other conditions that target pathways beyond GLP-1. This was complemented by a strategic collaboration with NVIDIA, leveraging advanced AI technologies to support future drug development.
With the launch of the NNPP, Novo Nordisk aims to not only optimise outcomes for individuals prescribed GLP-1RAs but also to solidify its leadership in the increasingly competitive obesity treatment landscape by embedding digital innovation across the full spectrum of care.
Read More
Leading health organisations release nutrition guidance for GLP-1 obesity therapies
Key Takeaways:
- Four major U.S. health organisations have released a joint clinical advisory detailing nutrition and lifestyle strategies to support people receiving GLP-1 receptor agonist (GLP-1RA) therapy for obesity.
- The guidance addresses both the therapeutic potential and risks of GLP-1 drugs, such as micronutrient deficiencies, muscle loss, and long-term adherence challenges.
- Eight evidence-based nutritional priorities are outlined, including personalised dietary planning, adequate protein intake, and integrated lifestyle support to improve outcomes and sustain benefits.
Introduction
In an unprecedented collaboration, four prominent American health organisations—the American College of Lifestyle Medicine (ACLM), the American Society for Nutrition (ASN), the Obesity Medicine Association (OMA), and The Obesity Society (TOS)—have released a joint clinical advisory titled “Nutritional Priorities to Support GLP-1 Therapy for Obesity.” Published across four leading peer-reviewed journals, the document presents consensus-driven guidance aimed at equipping clinicians with the tools to support people receiving GLP-1 receptor agonist (GLP-1RA) treatment with comprehensive, evidence-informed nutrition and behaviour strategies.
The Therapeutic Promise and Challenge of GLP-1RAs
GLP-1 therapies—comprising both mono- and combination agents—have become pivotal in modern obesity care. Clinical trials have demonstrated substantial placebo-adjusted weight loss outcomes, ranging from 5% to 18%, alongside significant metabolic, functional, and cardiovascular improvements.
Yet, experts caution that these results cannot be sustained through medication alone. As lead author Dr Dariush Mozaffarian of Tufts University noted:
“GLP-1s represent an important advancement in obesity care. But these medications can present challenges, including gastrointestinal side effects, risk of micronutrient deficiencies, muscle and bone loss, poor long-term adherence with subsequent weight regain, and high costs; and, on their own, are not enough. Nutrition therapy and lifestyle support are essential components to address these challenges, help patients maximise and maintain health gains over time, and ensure we are using these drugs wisely, effectively, and without bankrupting the healthcare system.”
Eight Nutritional Priorities to Support GLP-1 Therapy
The advisory sets out eight core nutritional priorities for clinicians managing people on GLP-1RA therapy:
- Patient-Centred Therapy Initiation – Considering individual goals, preferences, and medical history before prescribing.
- Baseline Nutritional Assessment – Evaluating dietary intake and nutritional status to identify existing deficiencies.
- Gastrointestinal Side Effect Management – Addressing common symptoms such as nausea or constipation that may deter adherence.
- Personalised, Nutrient-Dense Diets – Emphasising minimally processed foods tailored to the individual’s needs.
- Micronutrient Deficiency Prevention – Monitoring and supplementing as necessary to avoid complications.
- Adequate Protein Intake and Strength Training – Preserving lean body mass and preventing sarcopenia.
- Maximising Weight Loss via Diet Quality – Leveraging dietary composition to enhance the efficacy of pharmacotherapy.
- Supporting Broader Lifestyle Change – Integrating physical activity, sleep, mental health, substance use reduction, and social connection.
Evidence for Integrated Care
Several recent studies have reinforced the importance of combined treatment strategies. In research comparing pharmacological treatment alone with integrated care models—including structured nutrition support—people receiving both GLP-1 therapy and nutrition counselling achieved superior weight loss outcomes, greater adherence, and improved weight maintenance post-treatment (Wadden et al., 2021; Kushner et al., 2022).
Despite these promising findings, a significant implementation gap remains. Many individuals prescribed GLP-1RAs do not receive adequate dietary or behavioural guidance, leaving them vulnerable to avoidable adverse outcomes and reduced therapeutic benefit.
Addressing the Care Gap
John E. Courtney, PhD, Chief Executive Officer of the American Society for Nutrition, commented:
“GLP-1s are reshaping the landscape of obesity treatment, but it’s clear that medication alone is not a complete solution. This consensus-based guidance highlights the critical role of nutrition in supporting patients on GLP-1 therapy, with clear recommendations for health care providers to optimise outcomes, reduce risks, and fill urgent gaps in care through practical, evidence-informed nutrition strategies.”
The advisory encourages clinicians to implement a proactive, lifestyle-oriented approach. By prioritising nutrition and behaviour change alongside pharmacotherapy, clinicians can reduce risks such as gastrointestinal intolerance or micronutrient depletion, while enhancing patient outcomes and the cost-effectiveness of care.
A Scalable Strategy Amid a Growing Obesity Crisis
With obesity prevalence continuing to climb globally, the advisory positions integrated nutrition support as a scalable solution for improving the reach and sustainability of GLP-1-based therapies. The authors urge healthcare professionals to consider nutrition therapy and behavioural interventions as integral to every obesity care plan involving GLP-1RAs.
“Clinicians are encouraged to use the advisory’s tools and frameworks to help patients translate nutrition guidance into sustainable behaviours, making lifestyle medicine an active ingredient in every ‘prescription’ for obesity care.”
Publication and Upcoming Discussions
The joint advisory has been published concurrently in the following journals:
- American Journal of Lifestyle Medicine (ACLM)
- The American Journal of Clinical Nutrition (ASN)
- Obesity Pillars® (OMA)
- Obesity (TOS)
Further discussion will take place during the American Society for Nutrition’s annual meeting, NUTRITION 2025, held from 31 May to 3 June in Orlando, Florida:
- Fatima Cody Stanford, MD, will speak on Nutrition Considerations with Long-term Use of GLP-1RA on Saturday, 31 May (07:45–08:15 EDT).
- Monica Agarwal, MD, will present on Nutritional Priorities to Support GLP-1 Therapy for Weight Loss during the Energy and Macronutrient Metabolism (EMM) GEM Forum on Sunday, 1 June (15:05–15:20 EDT).
Conclusion
This advisory marks a critical step toward more holistic, patient-centred obesity care. By embedding evidence-based nutrition and behavioural support within GLP-1 therapy plans, clinicians can better safeguard against side effects, support long-term success, and elevate the standard of care for people living with obesity.
CCH Insight:
These guidelines are very important. They remind us that GLP-1 medications are not just about weight loss, but also about providing lasting health benefits for people living with obesity. This can only really be accomplished by combining the drugs with sustainable changes to diet and lifestyle, and most patients will need help to achieve this. The guidelines also remind us of the potential drawbacks of GLP-1 therapy, like nutrient deficiencies and muscle loss, and the importance of taking steps to minimise the risk of these through an integrated/multidisciplinary approach to obesity care.
Read More
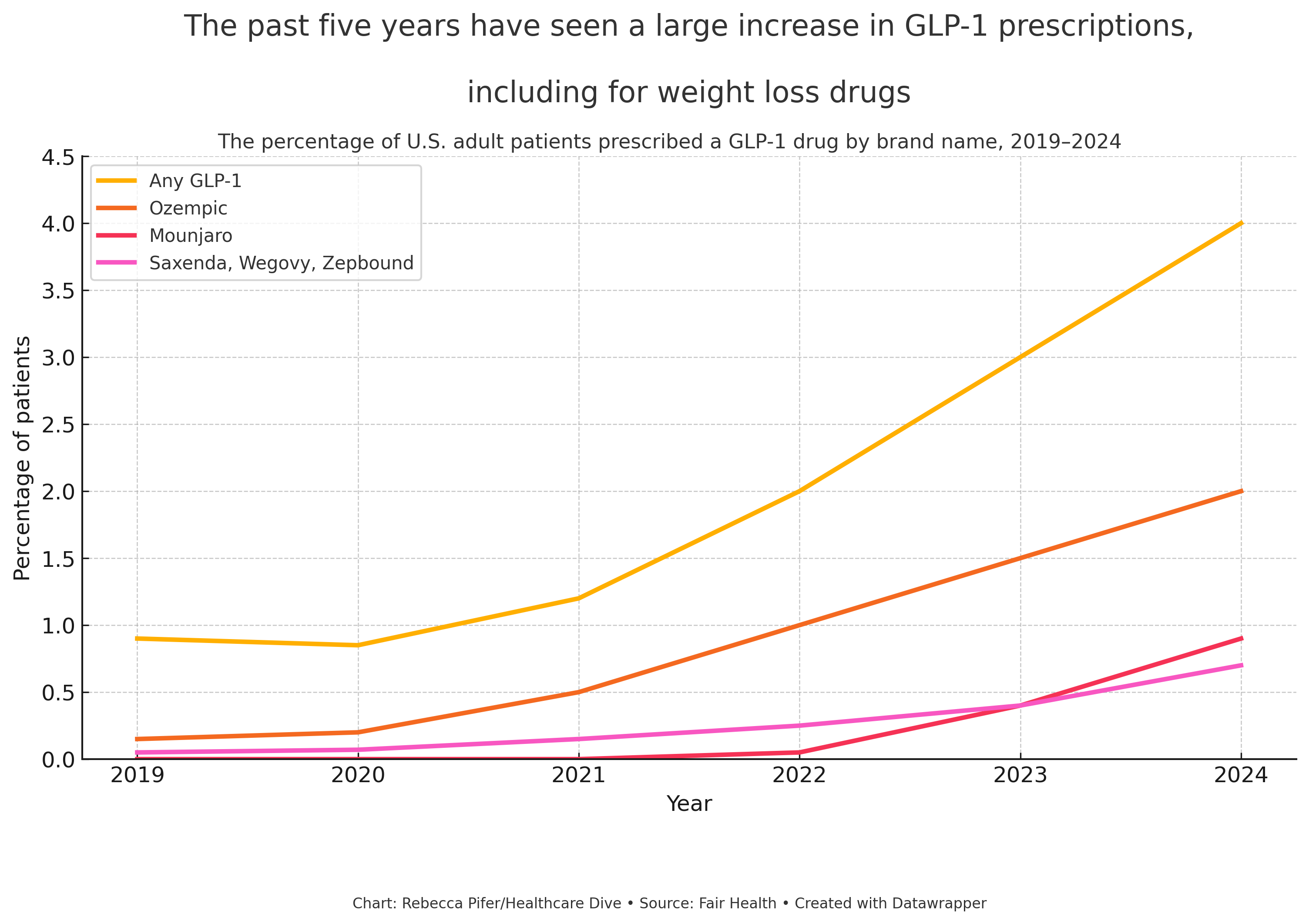
GLP-1 prescriptions for weight loss climb sharply, despite persistent barriers
Key Takeaways:
- GLP-1 prescriptions for weight loss have increased by nearly 2,000% among people without diabetes between 2019 and 2024, according to Fair Health data.
- Drugmakers face criticism and logistical challenges, including high costs, shortages, and concerns about replacing behavioural and surgical interventions.
- Government resistance to subsidising obesity medications and rising public scrutiny may slow broader uptake, despite clinical success and commercial demand.
Background: GLP-1 Receptor Agonists and Rising Obesity Treatment Demand
Glucagon-like peptide-1 receptor agonists (GLP-1 RAs) are a class of drugs that simulate a gut-derived hormone responsible for lowering blood glucose levels and suppressing appetite. Initially approved for the treatment of type 2 diabetes, these medications have more recently demonstrated efficacy in supporting weight loss. Their expansion into the field of obesity care has transformed both patient outcomes and the commercial pharmaceutical landscape.
Fair Health, a U.S.-based non-profit organisation, analysed over 51 billion commercial claims to identify trends related to GLP-1 prescriptions and obesity care. The data show a significant rise in GLP-1 prescriptions, particularly for weight loss purposes rather than diabetes management.
Explosive Uptake in Weight Loss Prescriptions
Among individuals prescribed GLP-1 medications in the past year, approximately half received the prescription for weight management, not for diabetes. When people living with type 2 diabetes were excluded from the dataset, the data revealed a 1,961% increase between 2019 and 2024 in prescriptions to individuals with overweight or obesity but without diabetes.
This staggering growth reflects both public demand and shifting clinical practice. GLP-1 RAs are increasingly viewed not only as antidiabetic medications, but as a frontline treatment option for obesity—a chronic and often intractable condition.
An Expanding Market and the Role of Industry
The commercial implications have been profound. Industry analysts project the anti-obesity drug market could exceed $100 billion globally by 2030. At present, three GLP-1 drugs are approved by the U.S. Food and Drug Administration (FDA) specifically for weight management:
- Saxenda (liraglutide) – Novo Nordisk
- Wegovy (semaglutide) – Novo Nordisk
- Zepbound (tirzepatide) – Eli Lilly
Although Saxenda received approval in 2014, it was not until Wegovy’s launch in 2021 that the weight loss potential of GLP-1s gained widespread public attention. Eli Lilly’s Zepbound followed and quickly contributed to $4.9 billion in sales in its first full year. In 2023, Novo Nordisk reported $9.9 billion in combined sales from Saxenda and Wegovy.
Shortages, Substitutes, and Setbacks
Rapid uptake led to supply shortages, during which telehealth companies partnered with compounding pharmacies to distribute non-branded formulations. Although these shortages have since resolved—restoring market exclusivity to the original manufacturers—the episode dented both projected 2025 revenues and investor confidence. It also contributed to leadership changes at Novo Nordisk.
Affordability and Access Barriers
The high cost of GLP-1 drugs remains a critical issue, with monthly list prices reported as follows:
- Wegovy: $1,350
- Zepbound: $1,060
(Source: Institute for Clinical and Economic Review)
Because long-term use is generally required to maintain weight loss, the financial burden on health plans is substantial. In 2024, fewer than 20% of employer-sponsored insurance plans covered GLP-1s for weight loss, largely due to cost constraints.
To address this, manufacturers have sought partnerships with major pharmacy benefit managers. Recent collaborations include:
- Novo Nordisk and Eli Lilly with Cigna’s health services subsidiary to offer discounts and cap out-of-pocket costs
- Novo Nordisk with CVS Caremark, granting Wegovy preferred formulary status
Policy Resistance and Political Backdrop
Obesity remains a public health emergency in the United States. According to the Centers for Disease Control and Prevention (CDC), over 40% of adults are currently living with obesity, a figure projected to reach 50% by 2030. Yet federal support for pharmacological obesity treatment remains limited.
Earlier this year, the Trump administration rejected a proposal to expand Medicare coverage to include anti-obesity drugs, a move that would have added $40 billion to taxpayer expenditures over ten years.
The decision coincides with political and cultural scrutiny of pharmaceutical interventions. Health and Human Services Secretary Robert F. Kennedy Jr. has been vocal in his opposition to pharmacological weight loss treatments, attributing rising obesity rates to poor dietary choices. He has argued that medication should not replace healthier food and lifestyle interventions.
“We cannot medicate our way out of a nutrition crisis,” Kennedy stated in a White House report released last week.
Impact on Other Forms of Obesity Care
Fair Health’s findings suggest that the rise in GLP-1 prescribing has coincided with a decline in bariatric surgery rates. This supports prior research indicating that patients are increasingly turning to pharmacotherapy instead of more invasive interventions.
However, the trend has also been linked to a reduction in behavioural health interventions, which raises significant clinical concerns. GLP-1s have been associated with increased risks of depression, anxiety, and suicidal ideation in some individuals, making ongoing psychological support an essential component of care.
Looking Ahead
While new partnerships and forthcoming price negotiations under the U.S. Inflation Reduction Act (effective 2027) may improve affordability—particularly for Medicare recipients—current dynamics underscore the complex interplay of clinical promise, economic burden, and political ideology.The rapid growth of GLP-1 prescribing marks a new chapter in the treatment of obesity. Yet its future success will depend not only on drug efficacy, but also on ensuring equitable access, maintaining comprehensive care, and fostering public trust in what remains a deeply politicised health issue.
Read More
GLP-1 receptor agonists show early promise in reducing BMI among children with severe obesity, study finds
Key Takeaways:
- GLP-1 receptor agonists appear to enhance treatment outcomes for children with severe obesity when added to existing intensive behavioural and lifestyle interventions.
- Clinically meaningful BMI reductions were observed in a higher proportion of children following the integration of GLP-1 medications into their care plans.
- Families reported additional benefits beyond weight loss, including reduced conflict around food and improved ability to follow lifestyle recommendations.
Background: Addressing Severe Obesity in Children
Children living with severe obesity face considerable health challenges and are at increased risk of metabolic and psychological complications. While glucagon-like peptide-1 (GLP-1) receptor agonists are now widely used to treat obesity in adults, their use in paediatric care remains a developing area.
These medications mimic the hormone GLP-1, which helps reduce appetite, prolong satiety, and slow gastric emptying. When prescribed as part of a holistic care plan, they may support young people in achieving clinically significant improvements in weight and health outcomes.
At the 2025 European Congress on Obesity (ECO), new data were presented suggesting that incorporating GLP-1 receptor agonists into childhood obesity treatment regimens could enhance the likelihood of meaningful BMI reduction.
The Study: Real-World Outcomes from Sweden’s National Childhood Obesity Centre
Dr Annika Janson and her research team at the National Childhood Obesity Centre, Karolinska University Hospital, Stockholm, investigated the real-world effects of GLP-1 receptor agonists when used in conjunction with intensive health behaviour and lifestyle treatment (IHBLT).
The retrospective study included 1,126 children aged 0–16 years (51.6% boys), all living with severe obesity as defined by the International Obesity Task Force criteria. Each participant was enrolled in the IHBLT programme, which involves a multidisciplinary approach to support children and their families in modifying lifestyle behaviours, such as:
- Healthy eating and nutrition education
- Managing meal portions and timing
- Reducing screen time
- Promoting physical activity
- Supporting psychological wellbeing
This intensive intervention is tailored in collaboration with families, schools, and other community stakeholders.
Introduction of GLP-1 Agonists into the Programme
From 2023 onwards, GLP-1 receptor agonists – initially liraglutide, later including semaglutide – were prescribed to approximately one in four children within the programme. The study aimed to determine whether adding these medications led to improved BMI outcomes, acknowledging the complexities and inconsistencies of medication use in real-world settings.
“GLP-1 drugs are increasingly used to treat obesity in adults. They can also be used in children from the age of 12 and clinical trials have shown children lose 5–16% of their body weight after a year of treatment,” said Dr Janson.
She also highlighted that real-life application presents challenges absent in clinical trials:
“Children have varying degrees of obesity, co-morbidities and complications and may have faced problems in supply of the drug, financing it or taking it. As a consequence, it is difficult to isolate the effect of adding GLP-1 drugs to the plethora of treatments that are already available.”
Findings: BMI Improvements and Emerging Trends
The study compared outcomes from children treated prior to 2023 with those treated during and after 2023, when GLP-1 drugs were introduced. Prior to 2023, the average BMI reduction across patients was relatively stable. However, among those treated in 2023, 30% of children achieved a clinically significant BMI reduction – defined as at least a 0.25 standard deviation drop – compared with 27% in previous years.
While the difference is modest, researchers believe it reflects a positive early trend.
“Only a fraction of the children had GLP-1 drugs and most of those who did started on them 6–12 months into the treatment programme,” explained Dr Janson. “Longer-term treatment may lead to greater improvements in BMI.”
Moreover, a point prevalence estimate from January 2025 found that approximately one quarter of the 2023 cohort were actively taking GLP-1 medications at that time.
“These are just early indications but it does look as if the average effect of being a patient at our clinic has improved after adding GLP-1 drugs to the toolbox,” she added.
Beyond BMI: Family Experiences and Behavioural Shifts
Notably, Dr Janson reported that families described benefits that extended beyond measurable weight outcomes.
“Many children with severe obesity describe hunger and a strong appetite – both of which GLP-1 receptor agonists are known to help with,” she said.
“Results beyond obesity are also important. The families reported reduced conflicts around food and improved capacity for other lifestyle adaptations. It was easier to stick to meals and limit snacks. Portions could be down-sized. For some children, not being hungry all the time is a new feeling.”
Conclusion: A Valuable Tool with Cautious Optimism
While not a universal solution, GLP-1 receptor agonists appear to be a promising adjunct in the care of children living with severe obesity. The study’s findings support their wider use, particularly when integrated within a comprehensive treatment plan.
“GLP-1 receptor agonists are clearly beneficial to many children with severe obesity and while they won’t help in all cases, more children should have access to these important medications,” Dr Janson concluded.
CCH Insight:
This study is a great example of how GLP-1RAs are meant to work. They are not, as some people think, a ‘lazy way’ or an ‘easy way’ to lose weight. They are a tool which, when used as part of a holistic care plan and supported by a multidisciplinary team, enables people (in this case children with severe obesity) to follow a healthier diet and lifestyle. The children were able to achieve this because GLP-1 medications modified their appetites, so they were no longer constantly hungry or thinking about food.
Read More
Weight-loss medications may halve risk of obesity-related cancers, landmark study reveals
Key Takeaways:
- GLP-1 receptor agonist medications may reduce the risk of obesity-related cancers by nearly 50%, rivalling the effects of bariatric surgery.
- The protective effects appear to extend beyond weight loss alone, potentially due to reductions in inflammation.
- Researchers and experts are calling for large-scale clinical trials to test weight-loss drugs as a new strategy for cancer prevention.
Introduction
A major new study suggests that weight-loss injections known as GLP-1 receptor agonists could nearly halve the risk of developing obesity-related cancers. Presented at the European Congress on Obesity in Málaga, Spain, and published in The Lancet’s eClinicalMedicine, the research has been described as “transformational” by leading cancer experts and may signal the beginning of a new era in preventive oncology.
Obesity, Cancer Risk, and Weight-Loss Interventions
Obesity is strongly linked with an increased risk of at least 13 different types of cancer. While losing weight is already known to reduce cancer risk, this study indicates that weight-loss medications may have protective effects that go beyond weight reduction alone.
The research, conducted by scientists in Israel, involved 6,000 adults with no previous cancer diagnoses. Participants had either undergone bariatric surgery or taken GLP-1 receptor agonists (GLP-1RAs), including liraglutide (Saxenda), exenatide (Byetta), or dulaglutide (Trulicity). These medications mimic the GLP-1 hormone, which plays a role in lowering blood sugar levels and promoting feelings of satiety.
Weight Loss vs Cancer Risk Reduction
Although participants who had undergone bariatric surgery lost approximately twice as much weight as those who used medication, both groups experienced a similar reduction in cancer risk. According to the study’s authors, bariatric surgery is associated with a 30–42% reduction in the risk of cancer. However, after adjusting for the greater weight loss associated with surgery, the protective effect of GLP-1 medications appeared stronger relative to the amount of weight lost.
Professor Dror Dicker, co-lead author of the study and head of internal medicine at Hasharon Hospital, Rabin Medical Center in Petah Tikva, Israel, commented:
“The protective effects of GLP-1RAs against obesity-related cancers likely arise from multiple mechanisms, including reducing inflammation.”
He also highlighted the potential of more advanced drugs:
“New generation, highly potent GLP-1RAs with higher efficacy in weight reduction may convey an even greater advantage in reducing the risk of obesity-related cancers, but future research is needed to make sure these drugs do not increase the risk for non-obesity-related cancers.”
Newer Medications Show Even Greater Promise
A second study, also presented at the European Congress on Obesity and published in the New England Journal of Medicine, compared different GLP-1 medications. It found that participants taking tirzepatide (sold as Mounjaro) lost around 50% more weight than those taking semaglutide (sold as Wegovy). Specifically, individuals using Mounjaro lost an average of 20.2% of their body weight, compared to 13.7% among those taking Wegovy.
Expert Reactions: A Transformational Moment
Professor Mark Lawler, an internationally recognised cancer researcher from Queen’s University Belfast, emphasised the significance of the findings:
“We already know bariatric surgery cuts obesity-related cancer risk by about a third; these data suggest target GLP-1s may cut that risk by nearly 50% – an approach that would be transformational in preventing obesity-related cancer.”
He continued:
“Biologically, this makes sense, as targeting GLP-1 dampens down inflammation, one of the hallmarks of cancer.
While further work is required on how it works, these data raise the intriguing possibility that a GLP-1 jab could prevent multiple cancers in the general population, including common cancers like breast and colorectal, and difficult to treat cancers like pancreatic and ovarian. This work could herald a whole new era of preventive cancer medicine.”
Professor Jason Halford, former president of the European Association for the Study of Obesity and head of psychology at the University of Leeds, proposed that GLP-1 drugs also be trialled in people with newly diagnosed cancer, to evaluate whether they could improve survival rates:
“The drugs have the potential to be a new dawn. And it’s not just prevention – weight management in people recently diagnosed with cancer is also critical in terms of outcomes. That would be the next thing to look at. More and more cancers are being associated with obesity.”
A Global Call to Action
In light of the findings, a coalition of 54 international experts from 12 countries released a joint statement at the conference urging that GLP-1 drugs be trialled urgently for cancer prevention. In response, a team of researchers at the University of Manchester, funded by Cancer Research UK, are planning a major clinical trial involving tens of thousands of participants. The study is anticipated to begin within the next three to five years.
Dr Matthew Harris, from the Manchester Cancer Research Centre, commented:
“Weight-loss jabs provide genuinely fantastic weight loss, and may provide an intervention that could be delivered on a population-scale, where we have not been able to achieve this before.”
Conclusion
This growing body of evidence suggests that GLP-1 receptor agonists may offer far more than just weight loss benefits. With their potential to dramatically reduce cancer risk, these medications could form the basis of a proactive, large-scale approach to cancer prevention, particularly for people living with obesity. Further clinical research will be critical to confirm these findings and determine the full scope of benefits—and risks—associated with long-term use.
Read More
NHS plans free weight-loss injections at community pharmacies
Key Takeaways:
- The NHS is preparing a trial to offer the weight-loss medication Mounjaro at community pharmacies, aiming to improve access and reduce waiting times.
- Pharmacies like Boots and Superdrug, which already sell these medications privately, may soon provide them free of charge under NHS schemes, particularly in deprived areas with high obesity rates.
- Experts stress the need for comprehensive support, including psychological and nutritional counselling, alongside the rollout of these powerful medications to ensure safe and effective use.
Weight-loss medications such as Mounjaro and Wegovy may soon be available free of charge at high street pharmacies as part of the NHS’s expanding efforts to address obesity in the United Kingdom.
At present, these medications are accessible only through specialist NHS weight-management clinics, which are hospital-run and face waiting lists extending up to two years. Consequently, although approximately 15 million people in Britain are classified as living with obesity and meet the eligibility criteria, only around 50,000 have been able to access these treatments through the NHS.
Currently, numerous pharmacy chains — including Boots and Superdrug — offer these medications privately at a cost of roughly £150 per month, but they are not available to NHS patients via this route.
In a move designed to speed up access, the government is preparing to launch a trial in which Mounjaro, the brand name for tirzepatide (manufactured by the US pharmaceutical company Eli Lilly), will be made available through NHS community pharmacies. The programme is expected to focus on deprived areas, where high unemployment and elevated rates of obesity intersect, with the broader goal of boosting economic growth by improving public health.
Due to the high workload already faced by general practitioners (GPs), community pharmacies are increasingly involved in prescribing medications — such as antibiotics — following brief consultations. A similar model is likely to be applied for dispensing weight-loss injections.
Clinical trials have shown that Mounjaro can help people lose, on average, 20 per cent of their body weight. In December of last year, the National Institute for Health and Care Excellence (Nice), the UK’s health watchdog, approved the medication for NHS use, explicitly stating that it could be administered not only in hospital clinics but also within GP surgeries or pharmacies.
The NHS is expected to release details in the coming weeks about how Mounjaro will be incorporated into community care pathways.
Dr Kath McCullough, NHS England’s national speciality adviser for obesity, described the move as an “exciting opportunity” and emphasised that the initiative is likely to concentrate on regions with the “greatest clinical need”. Speaking after the publication of the Nice guidelines, Dr McCullough stated:
“Community pharmacies already provide a range of care — some pharmacists who will go through, for example, your blood pressure medication with you and manage that. But it’s still early days and pharmacists prescribing weight-loss injections is one of several potential models that NHS England is exploring, and ultimately it will be down to each local ICB [integrated care board] to consider. The exciting thing here is that it’s pretty much uncharted territory.”
The Tony Blair Institute for Global Change, a think tank that holds significant influence with the Labour government, released a report last year arguing that the government’s prevention agenda would be “doomed to fail” unless weight-loss medications were delivered at scale. The report advocated for NHS partnerships with online pharmacies, rather than relying solely on specialist clinics, to expand access.
In addition, the UK government has partnered with Eli Lilly to conduct a five-year trial in Manchester, aiming to evaluate whether Mounjaro can support individuals in returning to work and in preventing obesity-related diseases, thereby alleviating strain on NHS resources.
Analysis conducted by Nice suggests that widespread use of the drug can result in substantial cost savings for the NHS, particularly by preventing conditions such as type 2 diabetes, which currently costs the health service £11.4 billion annually.
Prime Minister Sir Keir Starmer has previously remarked that weight-loss medications “could be very important for our economy and for health”. Health Secretary Wes Streeting has similarly commented that the new class of drugs could have a “monumental” impact on Britain’s productivity by reducing levels of worklessness.
While access to these medications on the NHS has been limited, more than half a million individuals in the United Kingdom are currently purchasing Mounjaro and Wegovy privately from online pharmacies.
Professor Jason Halford, representing the European Association for the Study of Obesity, expressed cautious optimism about the plans, stating:
“I welcome efforts to increase availability of these drugs, and pharmacies could certainly play a part in that.
The concern is getting enough support. People need close monitoring, psychological support and advice on nutrition.
Potentially this is certainly work that pharmacies could expand into, but these are powerful drugs and they do have side-effects. I would definitely welcome efforts to trial new ways to roll out the drugs.”
As this trial advances, experts, policymakers, and healthcare providers alike will need to ensure that access to these medications is paired with comprehensive support structures, helping individuals achieve sustainable, long-term health improvements.
CCH Insights:
This sounds like a great idea, to improve access to GLP-1RAs, particularly in areas of high deprivation. However, it needs to also provide the right kind of support for patients, and the necessary funding and training to deliver it. If you are spending taxpayers’ money on GLP-1 therapy, you need to make sure it is part of an integrated approach which optimises the safety of the patient and the likelihood the treatment will be successful. This means providing an integrated approach with things like nutrition advice, psychological support and monitoring of side effects. Pharmacists would require appropriate training and referral options to be able to deliver this kind of service.
This sounds like a great idea, to improve access to GLP-1RAs, particularlyin areas of high deprivation. However, it needs to also provide the right kind of support for patients, and the necessary funding and training to deliver it. If you are spending taxpayers’ money on GLP-1 therapy, you need to make sure it is part of an integrated approach which optimises the safety of the patient and the likelihood the treatment will be successful. This means providing an integrated approach with things like nutrition advice, psychological support and monitoring of side effects. Pharmacists would require appropriate training and referral options to beable to deliver this kind of service.
Read More
Antibiotic exposure before age two linked to increased risk of overweight and obesity in children
Key Takeaways:
- Antibiotic use within the first two years of life is associated with higher body mass index (BMI) and a significantly increased risk of overweight and obesity by age twelve.
- Antibiotic exposure before pregnancy, during pregnancy, or around the time of birth shows no statistically significant association with later childhood weight outcomes.
- Findings underscore the importance of careful antibiotic prescribing in early childhood, particularly avoiding unnecessary prescriptions for self-limiting conditions.
Children exposed to antibiotics during their first two years of life may face a heightened risk of developing overweight or obesity later in childhood, according to new research presented at the 2025 Paediatric Academic Societies (PAS) Meeting in Honolulu, Hawai‘i.
The study, led by investigators from the University of Oulu in Finland, specifically examined whether the timing of antibiotic exposure — ranging from before conception to early childhood — influenced weight outcomes in children. Researchers analysed data from 33,095 vaginally born children, drawing upon national health registers, medical records, and electronic growth charts to track weight development over time.
Early-Life Antibiotic Use Tied to Higher BMI and Obesity Risk
The research revealed that antibiotic use within the first 24 months of life was associated with significantly higher body mass index-for-age z-scores (zBMI) at two years of age. Children who received antibiotics during this window exhibited an average zBMI increase of 0.067 (95% confidence interval [CI]: 0.041 to 0.094) compared to children who were not exposed.
Long-term follow-up of these children up to the age of twelve showed that those who had received antibiotics in early life faced a 20% increased risk of developing obesity (adjusted hazard ratio [HR] 1.20; 95% CI, 1.10 to 1.31). Additionally, early antibiotic exposure was linked to a 9% increased risk of becoming overweight by age twelve. These associations persisted even after the researchers adjusted for several potential confounding variables, underscoring the robustness of the findings.
“Antibiotic exposure in the first two years of life has a stronger association with childhood weight gain than exposure during pregnancy stages or other early ages,” stated Sofia Ainonen, MD, PhD, a medical doctor at the University of Oulu and the study’s presenting author.
No Association Found from Maternal or Perinatal Exposure
The investigators also explored whether antibiotic exposure before conception, during pregnancy, or in the perinatal period influenced the likelihood of overweight or obesity in children. Their analysis indicated no statistically significant associations in these cases.
Within the study population, 39% of mothers had used antibiotics during the year preceding pregnancy, 27% during pregnancy itself, and 21% of children had been exposed during the perinatal period. However, none of these exposures were linked to higher BMI or weight-related outcomes later in childhood. This finding suggests that the critical window of influence may be limited to the early postnatal period.
Antibiotic Prescribing in Young Children Remains Widespread
Notably, the study found that 68% of the participating children had been prescribed antibiotics within their first two years of life, reflecting how common such early exposure remains. While antibiotics are essential for treating certain bacterial infections, they are frequently prescribed for conditions such as upper respiratory tract infections, where their clinical benefit may be minimal.
“Providers need to be cautious about prescribing antibiotics for young toddlers, especially unnecessary antibiotics for upper respiratory tract infections,” Ainonen emphasised.
Clinical and Research Implications
The findings contribute to a growing body of evidence indicating that the early postnatal period may represent a sensitive window during which antibiotic exposure can shape long-term health outcomes, including body weight regulation.
The study authors highlighted that future research aiming to uncover the biological mechanisms linking early antibiotic use to later obesity risk should concentrate specifically on the first two years of life, given the lack of associations found for exposures occurring before or during pregnancy.
Childhood obesity remains a critical global health challenge. As of 2022, more than 159 million school-aged children worldwide were diagnosed with obesity. The present study underscores the importance of antibiotic stewardship in early childhood as a potentially modifiable factor that could help reduce the long-term risk of overweight and obesity.
By focusing on appropriate prescribing practices and minimising unnecessary antibiotic use, especially during the crucial early years, healthcare providers may help support healthier long-term outcomes for children.
CCH Insight:
The results of this study are consistent with the increasing body of evidence that the gut microbiota plays a major role in metabolic health and conditions like obesity. A baby’s gut is sterile at birth, and then becomes populated with micro-organisms from its food and environment. This study supports the theory that oral ingestion of antibiotics during the first two years of life disrupts the establishment of a healthy gut microbiota and increases the risk of metabolic dysfunction and obesity.
Read More
Novo Nordisk introduces Wegovy to Thailand, marking first launch in Southeast Asia
Novo Nordisk has announced the launch of its highly popular weight management medication, Wegovy, in Thailand, according to an executive from the Danish pharmaceutical company’s local subsidiary. This development marks Wegovy’s first introduction into the Southeast Asian market.
Initially launched in 2021, Wegovy has significantly contributed to Novo Nordisk’s growth, propelling the company to become Europe’s most valuable publicly listed firm, reaching a peak valuation of $615 billion.
The medication, which is administered via injection, is now available in over a dozen countries, including the United States, Japan, and China. Thailand is the latest addition to this expanding list of markets.
“We actually received the Thai FDA approval already in 2023,” stated Enrico Canal Bruland, Vice President and General Manager of Novo Nordisk’s Thai subsidiary. He emphasised that Novo Nordisk had introduced Wegovy in Thailand ahead of the anticipated arrival of rival Eli Lilly’s weight management medication, Zepbound.
Bruland declined to disclose the pricing strategy for Wegovy within Thailand, a nation with an estimated population of approximately 66 million people. He also did not provide details regarding the company’s broader plans for expansion into additional Southeast Asian countries.
Currently, Wegovy is available for prescription at private hospitals across Thailand. Bruland confirmed that access would soon be extended to public hospitals, enhancing availability for a broader segment of the population.
“Over the last four years, we have invested approximately 500 million Thai baht in clinical trials in Thailand,” he noted, underscoring Novo Nordisk’s long-term commitment to the Thai healthcare landscape.
In addition to Wegovy, Novo Nordisk’s diabetes medication Ozempic, which contains the same active ingredient as Wegovy (semaglutide), is already accessible within Thailand’s healthcare system.
According to data from Thailand’s Ministry of Public Health, approximately 42% of adults in the country are living with obesity. The prevalence of obesity among school-aged children has also risen dramatically, increasing from 5.8% to 15% over the past two decades.
Reflecting on the economic burden of obesity, Bruland commented, “If we then look at the economic impact that this has, approximately 1 percent of GDP is used for health-related costs that come with obesity and productivity loss.”
He expressed optimism about Wegovy’s potential impact in Thailand, stating, “We believe with this innovation, we can make a big difference and hopefully bend this curve.”
Read More
Diabetes drug metformin reduces knee pain in people with overweight or obesity clinical trial shows
A widely prescribed diabetes medication may offer relief for people living with knee osteoarthritis (OA) and overweight or obesity, potentially delaying the need for knee replacement surgery, according to new research led by Monash University.
The clinical trial, published in the Journal of the American Medical Association (JAMA), found that metformin, a drug commonly used in the treatment of type 2 diabetes, significantly reduced knee arthritis pain over a six-month period.
The randomised, placebo-controlled study investigated whether metformin, compared to a placebo, could alleviate knee pain in individuals experiencing symptomatic knee osteoarthritis and who were living with overweight or obesity. Importantly, none of the participants had diabetes.
The research was conducted entirely within the community through telehealth consultations, making it accessible to participants across a range of locations. A total of 107 individuals (73 women and 34 men), with an average age of 60, were enrolled. Participants were randomised to receive either up to 2,000 mg of metformin daily or a placebo for six months.
Pain was assessed using a 0–100 scale, where 100 represents the worst imaginable pain. After six months, those in the metformin group reported an average reduction of 31.3 points, compared with an 18.9-point reduction in the placebo group—a difference considered to represent a moderate effect on pain.
“These results support use of metformin for treatment of symptomatic knee osteoarthritis in people with overweight or obesity,” the researchers concluded. “Because of the modest sample size, confirmation in a larger clinical trial is warranted.”
A New, Affordable Treatment Option
Professor Flavia Cicuttini, lead researcher and Head of Monash University’s Musculoskeletal Unit as well as Head of Rheumatology at The Alfred Hospital, described the findings as highly promising. She highlighted that metformin could represent an affordable, novel approach to improving knee pain in people living with knee osteoarthritis and overweight or obesity.
Current treatments for knee OA primarily focus on lifestyle modifications such as exercise and weight management, interventions that many patients find challenging to maintain. Medications such as paracetamol, topical anti-inflammatory creams, and oral anti-inflammatory drugs are also used; however, they often provide limited benefit and may not be suitable for everyone due to safety concerns.
Notably, no new drugs for osteoarthritis have been approved in Australia since the late 1990s, with the approvals of Celebrex (celecoxib) and Vioxx (rofecoxib).
Professor Cicuttini emphasised that treatment options for managing knee pain in osteoarthritis remain scarce. She noted that this scarcity often drives both patients and their doctors to consider surgical options prematurely.
This has led to a growing issue both within Australia and internationally, with rising rates of knee replacements being performed for earlier stages of osteoarthritis. This trend is underpinned by the belief that effective non-surgical treatments are lacking and that prosthetic knees have long lifespans.
“At first glance this may seem reasonable, but it is a major problem because patient dissatisfaction with knee replacements is already high at between 20–30%, even when the operation is technically perfect,” Professor Cicuttini explained. “Dissatisfaction rates are highest when the operation is done for early knee OA.
“To go through the effort and cost of a big operation like a knee replacement, only to be unhappy with the results because of ongoing pain and symptoms, is definitely low-quality care. Doing a knee replacement earlier also increases the potential need for the procedure to be redone.
“This costs about 3.5 times as much, so about $70,000 compared to $20,000, and the results tend not to be as good as the first time. The best outcome for patients is to delay the knee replacements until it is absolutely needed.”
How Metformin Could Change Knee OA Care
Professor Cicuttini noted that metformin could now offer general practitioners (GPs) an alternative strategy to recommend alongside lifestyle measures such as weight management and increasing physical activity.
“Metformin works in a number of ways on the knee, including affecting low-grade inflammation and other metabolic pathways that are important in knee OA,” she said. “It is a different way to treat knee OA pain.
“GPs are very familiar with metformin, which is a low-cost, safe medication. It could be provided to patients in addition to other treatments they use and has the potential to delay people having knee replacements before they are absolutely needed. If people on metformin have less knee pain and are able to do more physical activity, then knee replacements can wait.”
The fact that metformin is already well known to GPs, affordable, and has a strong safety profile strengthens its potential as an adjunct therapy. Furthermore, if individuals experience reduced pain and can be more active, this may lead to additional benefits in joint health, functional capacity, and overall wellbeing.
Next Steps: Integrating Metformin into Knee OA Management
Professor Cicuttini and her team are now collaborating with patients, GPs, orthopaedic surgeons, and other healthcare professionals to explore how metformin can be incorporated into clinical care pathways for knee OA. The aim is to enhance patient outcomes and more effectively target surgical interventions when they are truly necessary.
Metformin could be prescribed ‘off label’ for this purpose, following thorough discussions between patients and their healthcare providers. This approach would allow for careful consideration of individual circumstances and potential benefits.
“Metformin is safe and well tolerated,” Professor Cicuttini stated. “It is used safely in other non-diabetes conditions such as polycystic ovarian syndrome. Metformin could be provided simply and safely using a telehealth approach, as we did in our study, meaning that it could be provided across the community, including in regional and remote areas.”
The study represents an important step forward in addressing the unmet needs of people living with knee osteoarthritis and overweight or obesity, offering a promising, accessible solution that may improve quality of life and reduce the reliance on invasive surgeries.
Read More
Eli Lilly’s oral weight-loss drug matches Ozempic in trial results, signalling a shift in diabetes and obesity treatment
Eli Lilly’s experimental oral medication, orforglipron, has demonstrated weight-loss and blood sugar-lowering effects comparable to those of the blockbuster injectable drug Ozempic in a pivotal clinical trial involving individuals living with type 2 diabetes. The pharmaceutical company has announced its intention to seek regulatory approvals for orforglipron by the end of the year, aiming to introduce a new, more convenient option in a market currently dominated by injectable therapies.
News of the promising trial results sent Eli Lilly’s shares soaring by 16%, reflecting investor optimism around the drug’s commercial potential. Orforglipron is the first in a series of ongoing trials testing the oral treatment, and its success raises the prospect of a highly effective, user-friendly alternative to existing injectable weight-loss medications.
By contrast, shares of Novo Nordisk — the manufacturer of Ozempic — continued a downward trend, dropping by 7% on Thursday. Over the past year, Novo Nordisk’s U.S.-listed shares have fallen by more than 50%. In a research note, BMO Capital Markets analyst Evan Seigerman commented, “While Novo had the headstart… this first mover advantage has waned.”
The results from Lilly’s phase 3 clinical trial revealed that participants with type 2 diabetes taking orforglipron lost an average of 16 pounds — approximately 8% of their body weight — over a 40-week period. This surpasses outcomes observed with Ozempic, in which individuals on the highest dose typically lost around 6% of their body weight. Furthermore, Lilly indicated that weight loss had not plateaued by the end of the study period, suggesting that extended use could result in further weight reduction.
In terms of blood glucose control, orforglipron reduced haemoglobin A1c (HbA1c) levels — a key marker of long-term blood sugar — by an average of 1.3%. Although this falls short of Ozempic’s 2.1% reduction, the oral formulation’s overall benefits, including ease of use, are seen as significant.
Multiple pharmaceutical companies are currently in pursuit of effective oral weight-loss treatments, as global demand for such therapies accelerates. Forecasts estimate that the market for obesity drugs could exceed $150 billion in the coming years. With the publication of these results, Eli Lilly is now considered the frontrunner in the race to develop an oral alternative to injectable therapies.
Ozempic, which was first approved in 2017 for the treatment of type 2 diabetes, functions by mimicking the GLP-1 hormone — a naturally occurring hormone in the gut that helps regulate appetite and blood sugar. Eli Lilly’s existing injectable medication, tirzepatide, is marketed under the brand names Mounjaro (for diabetes) and Zepbound (for weight management). Tirzepatide mimics both GLP-1 and a second hormone, GIP, and has achieved weight reductions of up to 22% over 72 weeks in clinical studies.
Unlike tirzepatide, orforglipron targets only the GLP-1 pathway. However, its distinction lies in its composition: it is a synthetic small molecule, not a peptide-based drug. This molecular structure allows for simpler and more scalable manufacturing, which could enable broader access to effective weight-loss treatment.
“Readily manufactured” oral agents like orforglipron may dramatically expand access to treatment, particularly among individuals who face barriers to injectable therapies. Lilly also reported that orforglipron’s safety profile was consistent with other GLP-1 receptor agonists, easing concerns that side effects could hinder its commercial viability.
“The data is fantastic from an efficacy standpoint,” said Kevin Gade, Chief Operating Officer at investment firm Bahl & Gaynor, which holds shares in Lilly.
The company has also confirmed that it will publish results from another trial focused specifically on weight management later this year. Regulatory submissions for approval to treat obesity are expected before the year’s end, with an application for diabetes to follow in 2026.
“While this trial alone is very good, this just bodes extremely well for their trial in obesity patients,” Gade added.
Regarding side effects, the trial found that 13% to 18% of participants experienced nausea at varying doses, compared to 2% of those given a placebo. Diarrhoea occurred in 19% to 26% of individuals on orforglipron, and vomiting affected between 5% and 14%, depending on the dose.
“These results firmly validate the tolerable profile of orforglipron,” Seigerman noted in his analysis.
Importantly, Lilly reported no signs of liver-related safety issues in its trial. This stands in contrast to Pfizer’s recent announcement that it would halt development of its experimental weight-loss pill, danuglipron, after a participant in one of its trials experienced potential drug-induced liver injury — a side effect which resolved after discontinuing the medication.
Lilly did state that 8% of patients on the highest orforglipron dose discontinued treatment due to adverse events. However, reductions in HbA1c across all tested doses ranged between 1.3% and 1.6%, reinforcing the drug’s effectiveness in managing blood glucose levels.
The trial’s multi-dose data revealed that individuals taking orforglipron daily achieved the following average reductions in body weight over 40 weeks:
- 4.7% reduction with a 3 mg dose
- 6.1% reduction with a 12 mg dose
- 7.9% reduction with a 36 mg dose
By comparison, individuals given a placebo experienced a 1.6% reduction in body weight.
Lilly has expressed confidence in its ability to meet global demand for orforglipron, should regulatory approvals be granted. The company noted that it recorded $550 million in drug-related inventory in its February financial statements, underscoring its readiness to launch the medication on a global scale.
If successful, orforglipron could become a landmark treatment option for people living with type 2 diabetes and obesity — offering meaningful weight loss in a daily oral format, with manufacturing and access advantages that may redefine the future of obesity care.
Read More